Xujun Duan wants to find new treatments for autism.
In service of that quest, Duan, professor of biomedical engineering at the University of Electronic Science and Technology of China in Chengdu, has spent most of the past decade studying how the brains of autistic people differ from those of non-autistic people. Functional connectivity between the medial prefrontal cortex and the amygdala, as well as other regions of the so-called “social brain,” seems particularly low in autism, Duan and her colleagues have reported.
That suggested to Duan that functional connectivity of the amygdala might be a good target for transcranial magnetic stimulation (TMS), which involves generating a magnetic field close to the head to alter neuronal activity. Nudging an autistic person’s amygdala toward more typical activity patterns might ease their social difficulties, she hypothesized.
Researchers have previously explored using TMS to treat autism, but the evidence is thin. Some studies have shown the treatment to ease repetitive behaviors or social difficulties, whereas others have not. According to a 2020 review of the use of TMS in autism, only 9 of the 23 studies assessed included any randomization or placebo group, making it difficult to gauge the technology’s effects. What’s more, it is unclear how the magnetic stimulation might work to modulate brain activity in the first place.
Duan and her colleagues hypothesize that personalized targeting may improve the effects of TMS. The amygdala is located deep in the brain, she says, making it a challenging region to reach with a noninvasive approach. So in a recent small clinical trial, Duan and her colleagues imaged the brain of each participant to identify which networks have strong functional connectivity with the amygdala. They then attempted to indirectly stimulate the amygdala via TMS by targeting the magnetic fields to those more accessible networks. The results of the trial, which she presented at the Organization for Human Brain Mapping meeting in Montreal, Canada, in July, have not yet been published.
Spectrum spoke with Duan about that clinical trial and the questions that remain about TMS and autism.
This interview has been edited for length and clarity.
Spectrum: How does your approach differ from how TMS has been used in the past?
Xujun Duan: Most previous studies used TMS to target the prefrontal cortex to treat executive function in autism. Or they targeted the motor cortex to treat sensorimotor function, or the temporal parietal junction, which is one of the regions in the social brain. But those studies did not use imaging to guide their treatment. They also did not have any imaging data to measure changes in brain function after the treatment.
In our recent clinical trial, we scanned the participants before the treatment, which enabled us to find the best stimulation site for each person. And we also scanned them after the treatment. That let us see what happened inside the brain — and how the relationship between the brain and the behavior changed.
S: Can you tell me more about your clinical trial?
XD: We recruited autistic children, ages 3 to 7 years old. Most of them have severe autism — they have a very low IQ; they have very minimal verbal ability. We conducted a double-blind, randomized trial with two groups: Around 20 received imaging-guided stimulation of the amygdala, and 20 received stimulation of the dorsolateral prefrontal cortex (DLPFC), which is a brain region that has been used as a TMS target in the past. All participants were treated for a total of 20 days — 5 days a week.
S: What did you find?
XD: A professional clinician used the Autism Diagnostic Observation Schedule (ADOS) to assess each participant’s autism traits before and after treatment, and we found that, for the amygdala-targeted group, they had a significant improvement in their ADOS score related to social and communication skills. But we did not see that change in the DLPFC-targeted group.
The amygdala group also had overall improvement on parent-reported questionnaires, but the DLPFC group did not. For the DLPFC group, we only found a significant improvement for parent-reported signs of depression.
Lastly, we found that, for the amygdala group, when the children were viewing a picture of a face, they had increased eye fixation counts on the eyes and face areas, meaning that after the treatment, they are paying more attention to social stimuli than they were before.
S: What did you see when you imaged the participants’ brains?
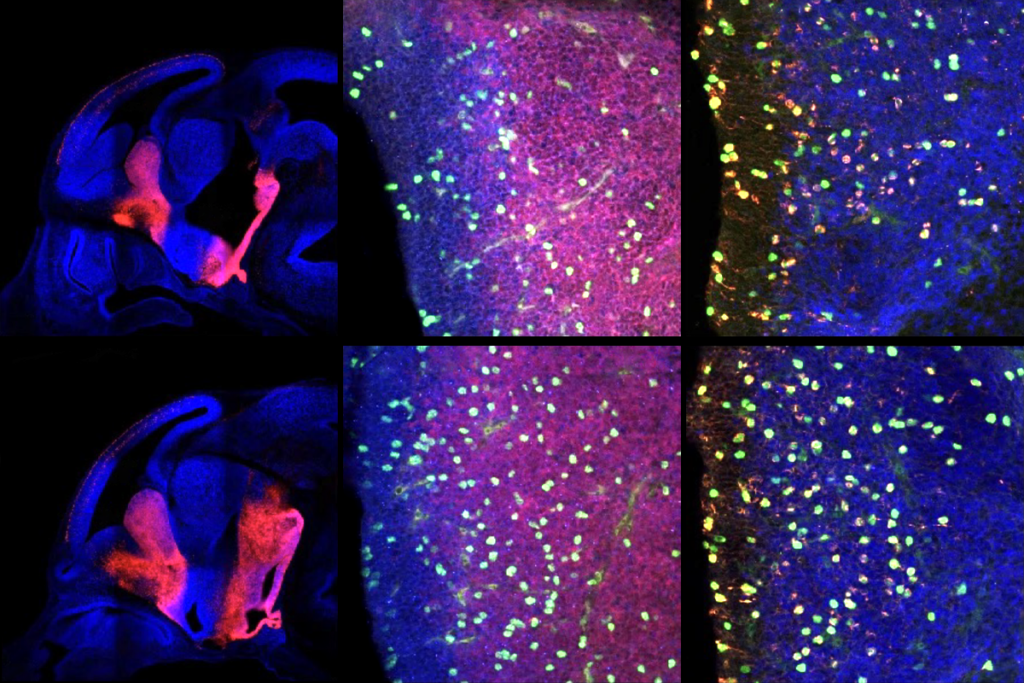
XD: Before treatment, we had found that the autistic children had increased amygdala gray-matter volume, on average, compared with neurotypical controls. And after the treatment, we found that the gray matter of the amygdala had decreased for the amygdala-targeted group. We also looked at functional changes in the brain, and we found that the activity of the amygdala also decreased following treatment.
We did not find any relationship between those amygdala changes and the participants’ behavioral changes. But we did find that changes in the connectivity between the amygdala and other networks correlated with the improvement in social and communication skills in the amygdala-targeted group. And that makes sense, because our behaviors stem from the function of many brain regions that might be associated with changes in the amygdala.
S: How long does the effect last?
XD: We were planning to conduct a follow-up assessment after one or two months. But actually, because of the COVID-19 shutdown, we were unable to have the families come back. We do have several parent rating scales that suggest that about one month after the treatment, the effect still exists. But our brain has lots of plasticity, and we do not know at this point if the changes to gray-matter volume of the amygdala might remain.
S: What are the next steps?
XD: We have no idea the mechanism behind the results, or whether it is a good treatment for most autistic children. We still need lots of other follow-up studies — maybe animal studies — to look at the effects, to look at the mechanisms and understand why this stimulation can reduce a region’s gray-matter volume.
S: What do you hope other researchers take away from your findings?
XD: I think that we should consider that the amygdala, or the social brain, might be a very effective target for treatment — not only for TMS, but also for other therapies.