This article is more than five years old.
Neuroscience—and science in general—is constantly evolving, so older articles may contain information or theories that have been reevaluated since their original publication date.

Experimental surgeries to prevent seizures may help scientists understand the link between autism and epilepsy.
D
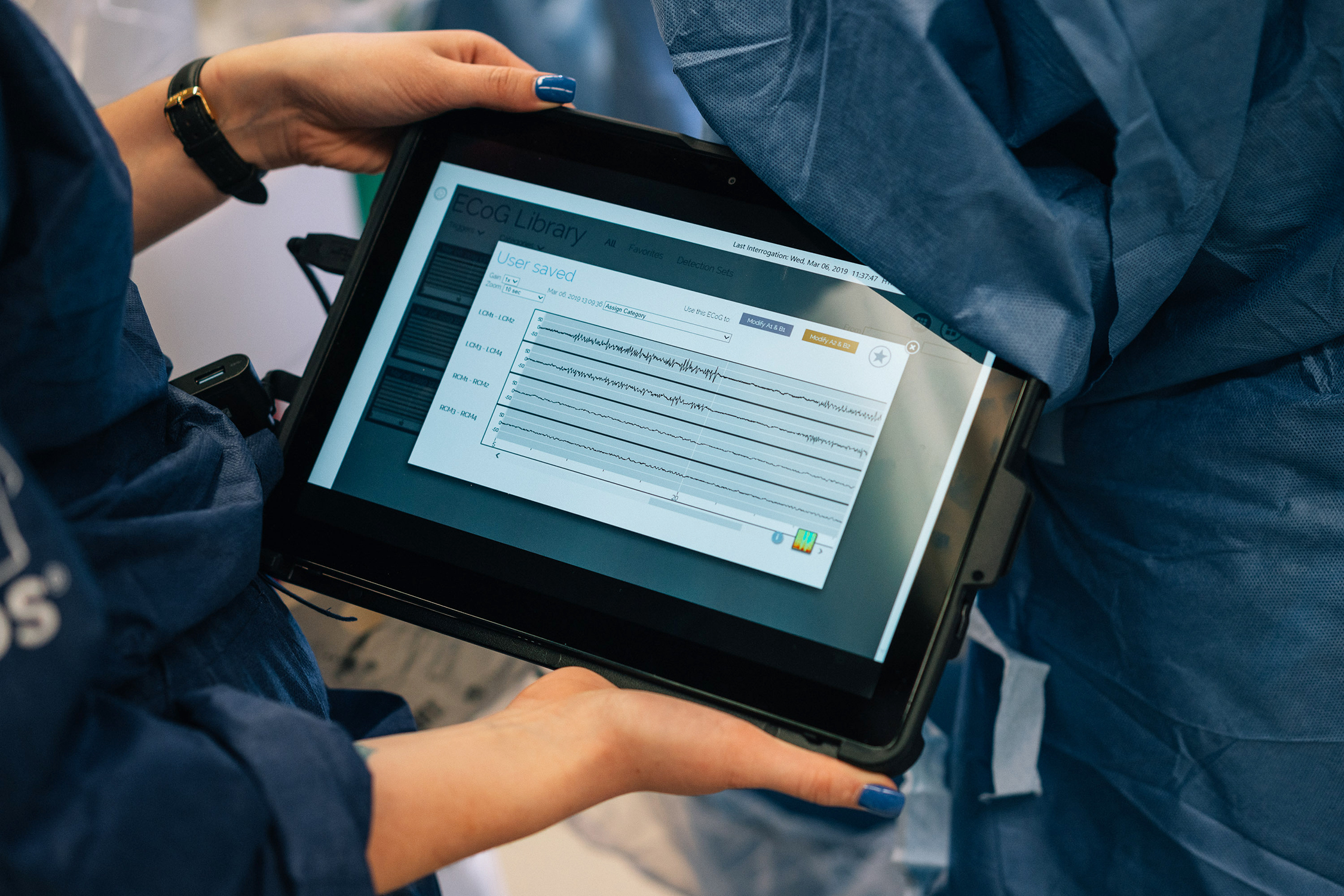
elicate lines dance across a screen mounted on the wall of the operating room. Their peaks and valleys become pronounced, suddenly flatten into a straight line — and then return, stronger than before.These digital traces represent the buzz of neurons in 12-year-old Kevin Lightner, read by two thin electrodes that surgeons have inserted deep into his brain. Kevin, who has autism and has had seizures since he was 8 years old, lies uncharacteristically still in the center of the room, draped under a blue sheet, his tiger-print pajamas neatly folded on a nearby shelf.
What’s happening in this room may be the last chance to bring Kevin’s seizures under control.
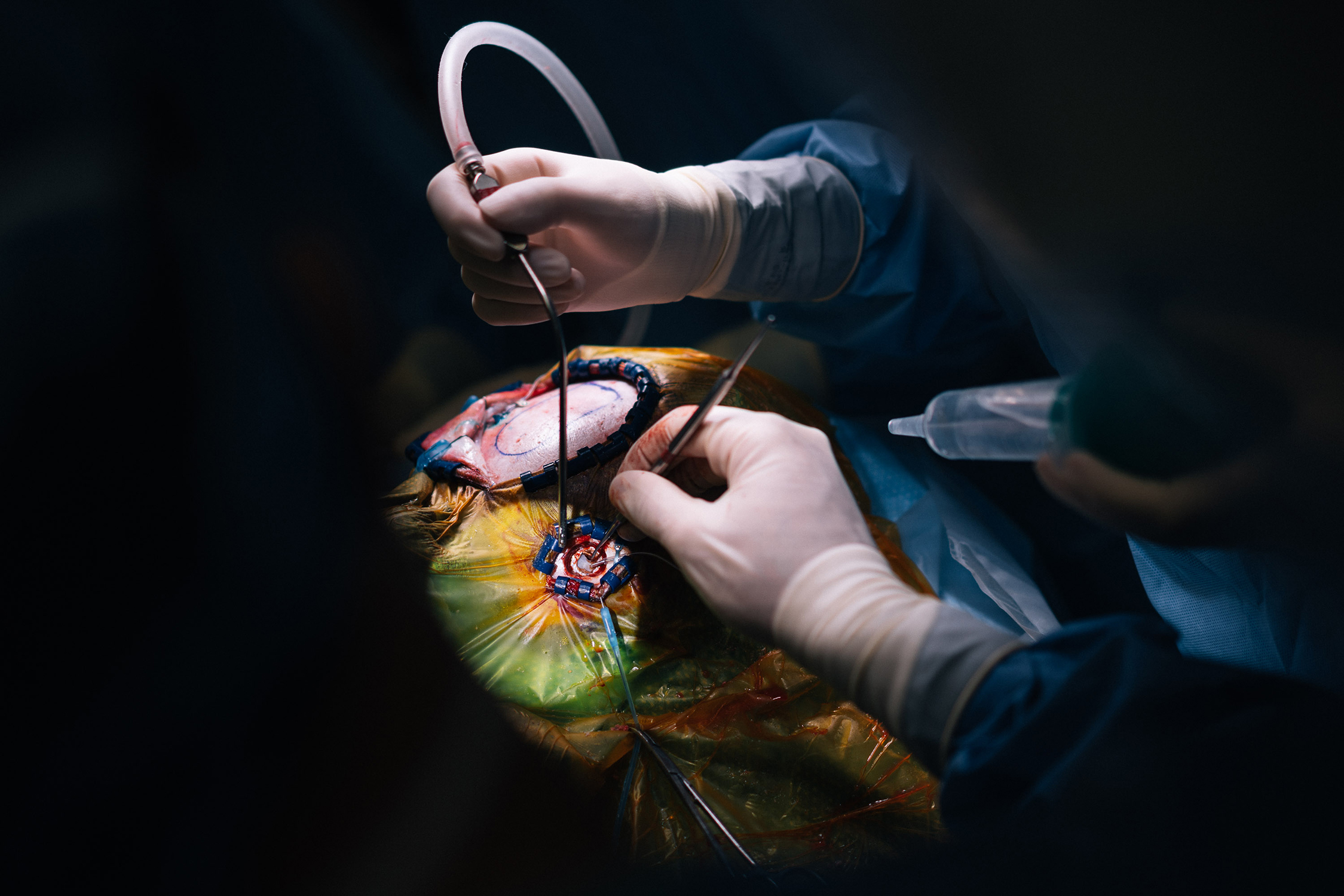
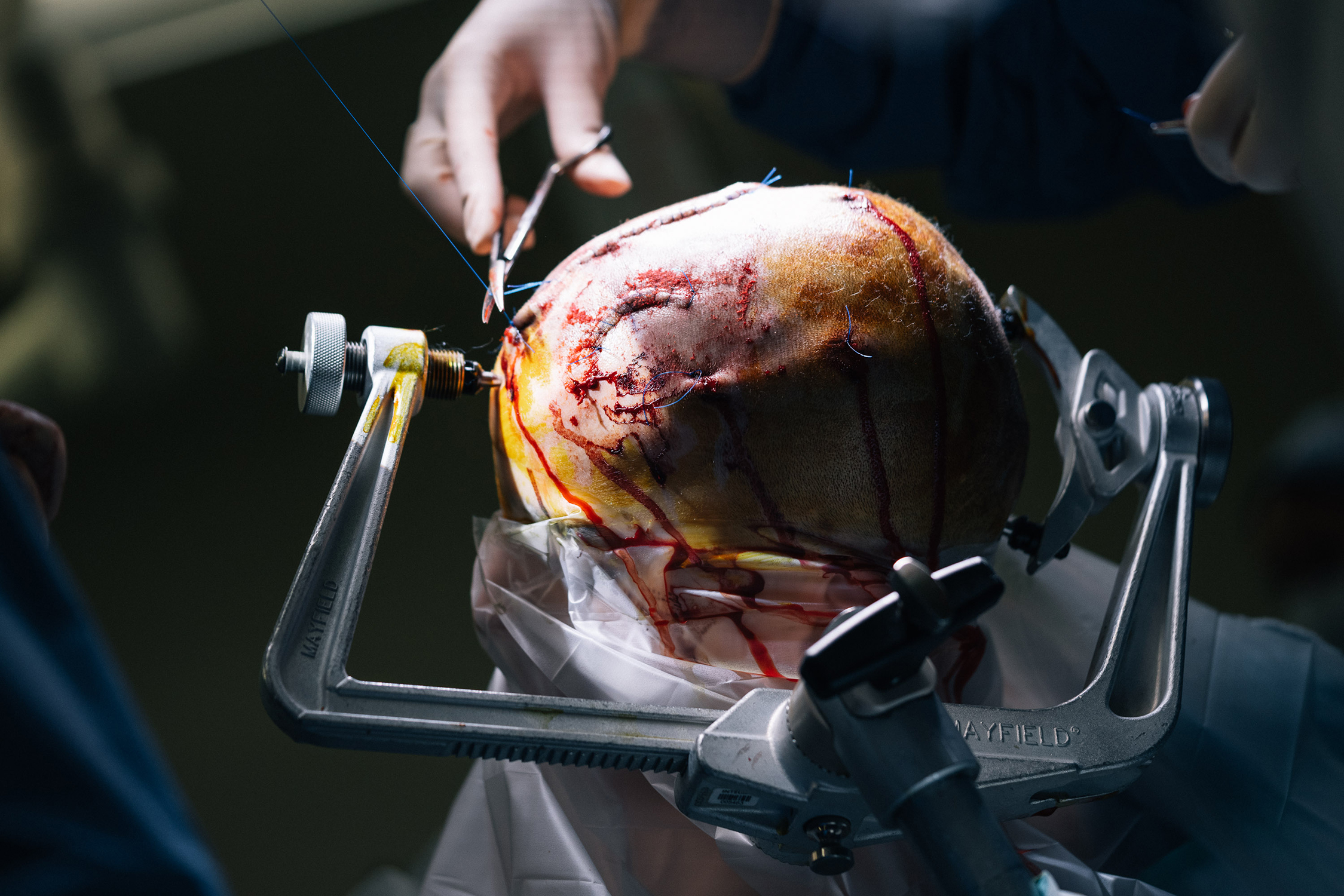
An hour and a half ago, neurosurgeon Saadi Ghatan removed a roughly 2-inch by 1-inch piece of the top of Kevin’s skull. He replaced it with a rectangular metal device, carefully screwed into the newly exposed edges of bone. The implant, a ‘responsive neurostimulation device,’ is now transmitting signals from the electrodes planted in Kevin’s thalamus. The surgeons’ hope is that the device will learn to recognize what kind of brain activity precedes Kevin’s seizures and discharge electrical pulses to prevent them — like a “defibrillator for the brain,” as Ghatan puts it. If it works, it could save Kevin’s life.
Ghatan projects the device’s readout to the screen by gently placing a black wand over the exposed metal in Kevin’s skull. The signal on the screen is surprisingly strong, given that it stems from the thalamus, a brain region that reveals its activity only weakly, if at all — and so is rarely the choice for monitoring seizures.
The rapid spiking with pauses in between echoes electroencephalograph readings the team took of Kevin’s brain before surgery. The pattern is “classic Kevin,” says his neurologist, Madeline Fields, who has donned scrubs for the first time in more than a year to get this glimpse into his brain.
Kevin was an infant when his mother, Lisa Lightner, learned he has dup15q syndrome, a genetic condition that causes epilepsy, intellectual disability and autism. Multiple types and combinations of drugs — what Lightner calls “the medication dance” — did nothing to mitigate Kevin’s seizures. Looming in Lightner’s mind were five terrifying letters: SUDEP, or sudden unexpected death in epilepsy, a constant threat to her child’s life.
Her fear led her to look for other treatments for epilepsy, and eventually to surgery. Some doctors recommended severing the two halves of Kevin’s brain to prevent seizures spreading from one side of the brain to the other. But Lightner knew two children in whom that approach had failed, and whose parents regretted opting for it. She then stumbled across a small study showing that the stimulation device lowers the odds of sudden death. After vetting surgeons in Philadelphia and Boston, Lightner sought out Ghatan, one of the few doctors in the United States who implants the device in children.
The procedure is still experimental. When the origins of epilepsy are clear, surgeons typically remove the tissue involved. But some autistic children, like Kevin, are not candidates for this because the source of their seizures in the brain is unclear. Ghatan started using the new approach to help these children four years ago. The results have been promising but limited, Ghatan says. “It’s not anything that can hold up yet from a scientific perspective.”
As he and others chart the outcome of these surgeries, though, they might learn how autism and epilepsy are related, a lingering question in the field: About one in four autistic children older than 13 also has epilepsy; conversely, having epilepsy increases the chance of an autism diagnosis roughly 10-fold. A preponderance of evidence suggests the two conditions have common genetic origins. But does epilepsy cause autism or at least alter its course? These surgeries might answer that question.
If the answer is yes, it adds urgency to the need to help children like Kevin: The sooner these children’s seizures can be brought under control, the better they are likely to fare long term.








Pre-op pep talk: Kevin Lightner gets support from his father before his experimental epilepsy surgery.
Scrubbed in: Doctors in the operating room prepare for the painstaking procedure.
Small window: The surgeon cuts out a piece of bone from Kevin’s skull to make room for an implant that prevents seizures.
Delicate handiwork: Thin electrodes pass through brain regions responsible for thought, planning and memory.
Tucked in: The implant screws directly into Kevin’s skull to keep it in place, with extra wires at the top in case they are needed later.
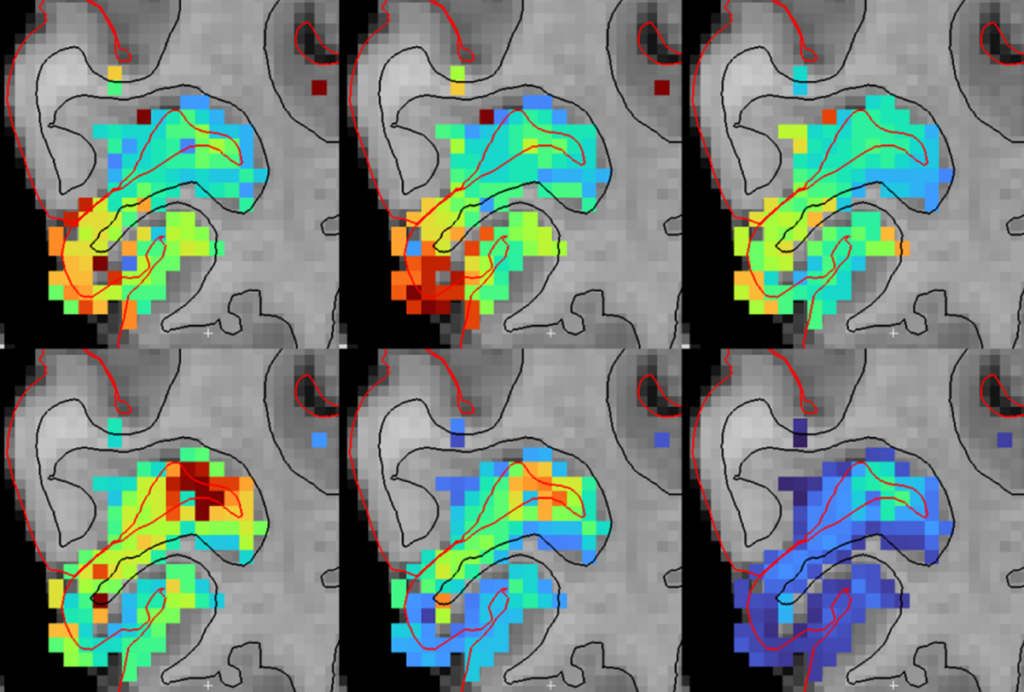
Charted paths: The surgeons follow preplanned trajectories, shown on the monitor, to feed the electrodes into Kevin’s brain.
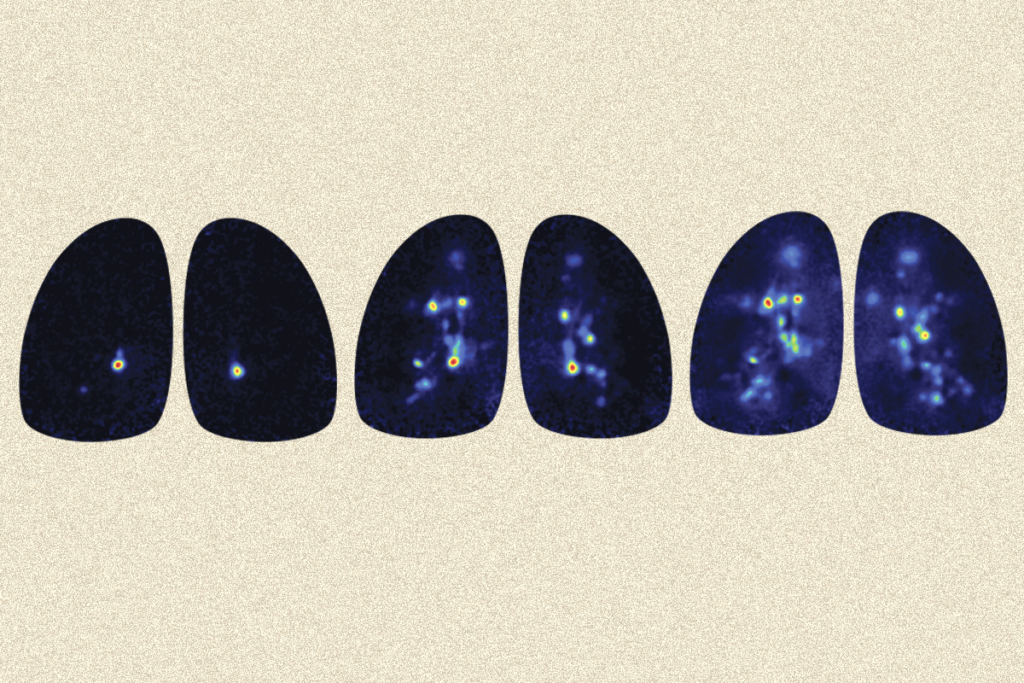
Rapid spiking: The readout of Kevin’s brain activity reveals that his thalamus, which acts as a signal relay center, is unusually active.
Closing time: A small bulge remains after surgeons close Kevin’s scalp over the implant.
Handle with care: Saadi Ghatan, the neurosurgeon, cradles Kevin’s head.
Cautious optimism: After a successful operation, Ghatan still has “a hundred years’ worth of anxieties,” he says.
Long wait: Kevin’s parents receive news about the procedure.
B
efore Kevin turned 8, the Lightners woke up every day thankful that he didn’t have the seizures that often plague children with dup15q syndrome. They took him to visit his favorite Sesame Street characters, Count von Count and Oscar the Grouch, at a local amusement park. Kevin ran races in the Special Olympics, joined in on weekly school outings to the grocery store or local farms, and enjoyed family vacations at the beach. Although he could not speak much, he often repeated single words, such as ‘yes’ and ‘no.’Then, early one morning in July 2015, Lightner heard a loud thud from the boy’s room. She found him lying on the floor convulsing. After that first episode, he “went from zero to full throttle in a matter of weeks,” Lightner recalls. As the number of seizures increased, Kevin shrank, both in stature and spirit: He spent his days hunched in a wheelchair and in a helmet to protect him from sudden falls. He stopped speaking. At school, his full-time aide spent all her time keeping him safe, and so he stopped learning as well. By the day of his surgery, Kevin was having more than 50 seizures a day.
The morning of his surgery at Mount Sinai Hospital in New York City, Kevin sat on a cot outside the operating room. He was a whirlwind of motion, rocking back and forth and twisting from side to side. His father, Dan Lightner, listened intently to Ghatan while keeping one hand protectively on Kevin. More than once, Dan turned away from Ghatan to fold Kevin’s jerking head in a protective embrace. Kevin seemed unaware of why he was there or of anything going on around him. Even so, when he knocked his Count von Count doll off the edge of the bed, he abruptly stopped rocking and returned it to safety. That swift, precise motion offered a glimpse of the Kevin his mother talks about before seizures overwhelmed his brain.
Seizures can start at any time in autistic children, but there are two periods that are particularly common: early childhood and adolescence. For adolescents, the onset of seizures can temporarily sideline parts of the brain, preventing and even counteracting the learning that can help to temper their autism traits. Neurologist Orrin Devinsky says some seizures are akin to people who are so distracting that they stop you from completing a task: The brain tissue involved is not only unavailable for anything else, it also throws the rest of the brain off-kilter.
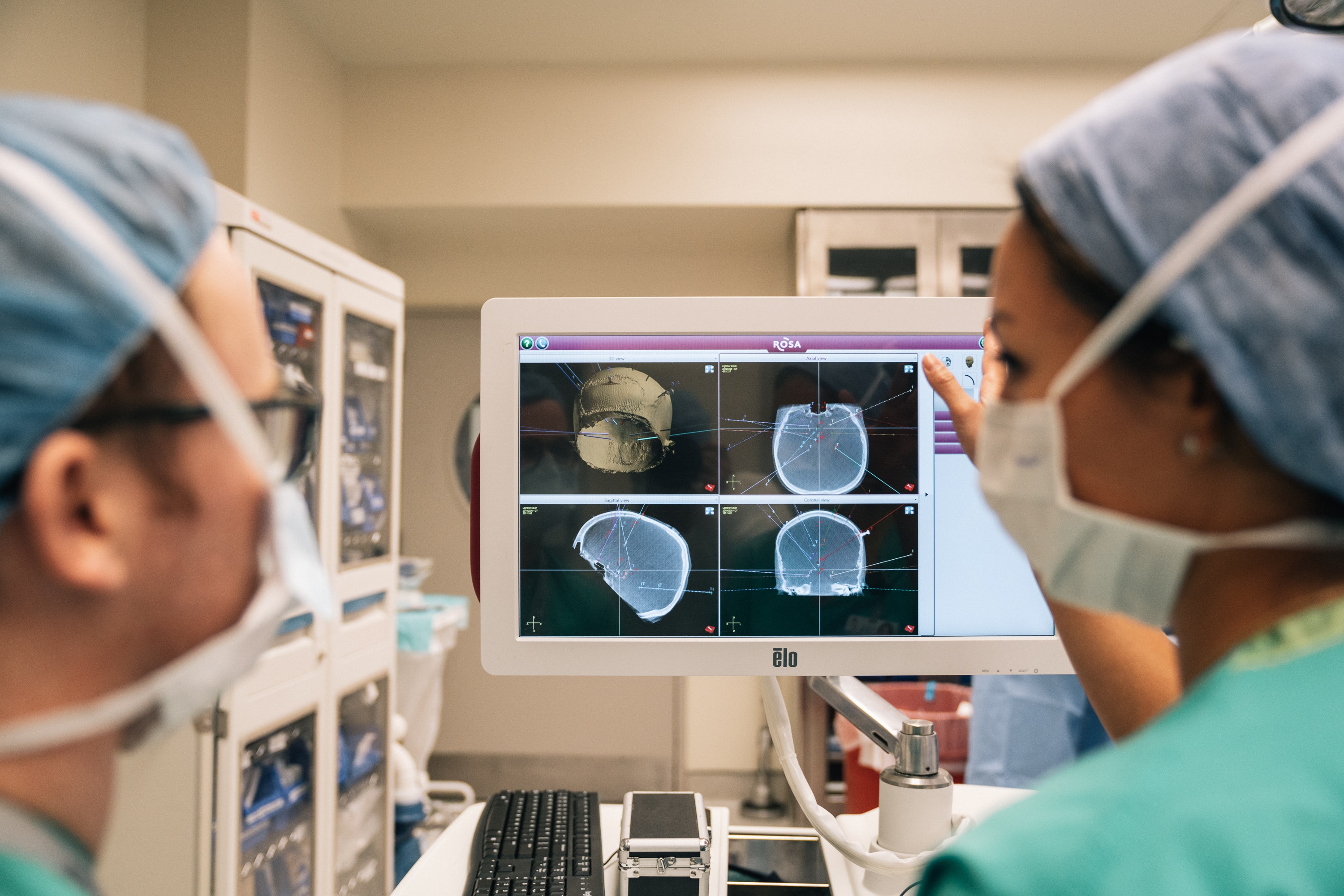
Careful alignment: Brain scans help doctors plan the electrodes’ path into Kevin’s brain.
The effect of this disruption may be long-lasting when seizures begin in early childhood or infancy, experts say, as is often the case in tuberous sclerosis, a condition related to autism. Infantile spasms — severe seizures that begin in the first year of life — might alter development and lead to some autism traits, and even autism itself. Understanding this link could have profound effects on clinical treatment, says Judy Liu, a neurologist at Brown University in Providence, Rhode Island. “If it turns out that seizures, the abnormal activity itself, is damaging the hippocampus or other brain structures, then it means that clinicians have to be even more aggressive in treating seizures — not just for tuberous sclerosis but for all forms of autism,” Liu says.
Studying children with tuberous sclerosis offers an opportunity to understand the condition’s link to autism. Because researchers can diagnose tuberous sclerosis early, even in utero, they can track these children from birth. So far, they have found that roughly half of the children are later diagnosed with autism, and 80 percent have epilepsy. Those who have seizures before age 1 have worse cognitive skills than those who are spared seizures, or who begin to have them later.
One team is testing whether preventing seizures can ease autism traits in these children. “Tuberous sclerosis is kind of a model genetic condition because there’s such a high rate of autism within the genetic diagnosis. We’re after the holy grail, if you would say, in terms of impacting the risk for epilepsy in a positive way,” says lead researcher Martina Bebin, professor of neurology at the University of Alabama in Birmingham. Bebin and her colleagues are scanning the brains of children with tuberous sclerosis, starting at birth, using an electroencephalogram every six weeks. (They have enrolled more than 70 children so far and plan to enroll 80.) They have already identified a pattern of activity that augurs imminent seizures. They give children with this signature a moderate dose of the epilepsy drug vigabatrin; the other children act as controls. When children in either group have a first seizure, doctors administer a high dose of vigabatrin to treat them.
As part of the trial, the researchers assess the children’s development at 6, 12, 24 and 36 months of age, with autism screening at the latter two ages. They have yet to analyze the results. But another study by a different team showed that at a 30-month follow-up, none of the 10 children they treated with vigabatrin were diagnosed with autism.
“One of the big questions we have is how does [epilepsy] influence developmental outcome?” Bebin says. “We have some inkling that it does, but we’ve never been able to get on the preventative side of this to really have a clear picture of the impact.”
S
eizure control can make an enormous difference to autistic people’s lives, regardless of its impact on diagnosis. Put simply, “seizures cause neuronal firing, and that can drown out or derail normal development of the brain,” says Anne Berg, research professor of pediatrics at Northwestern University in Chicago, Illinois.In a 2017 study, Ghatan and his colleagues reported that traditional epilepsy surgery improved social behavior and communication and eased aggression in many of the 56 autistic people they treated. Surgery also seems to foster long-term improvements in social behavior, cognition and language in people with severe epilepsy.
When Fábio Rocha’s psychologist diagnosed him with autism in his 20s, it finally explained Rocha’s introversion, as well as his sensitivity to high-pitched sounds and to blue or white lights. “Interactions with people used to be very, very unpleasant — very unpleasant. I was not sure what to say; I was not sure what a person was trying to say to me,” he recalls. “I did not understand jokes most of the time. They meant nothing to me at all.” He was so unhappy that he began to use alcohol to dull his anxiety and sensory overload, and he even attempted suicide.
Rocha has unusual seizures that elevate his heart rate, blur his vision and cause his fingers and tongue to tingle. A doctor prescribed him the anticonvulsant lamotrigine, which stopped them. To Rocha’s surprise, when his seizures stopped, other people started to make more sense too. “[Before,] I would pay more attention to the sound of the words than to the meaning of the words,” he says. “When I’m medicated, I’m able to block out this distraction and pay attention so I can actually hear what people are trying to say to me.” Now 27, Rocha is doing well in his third year of medical school.
Many clinicians know of dozens of cases like Rocha. Neurologist Nancy Minshew recalls an autistic child who was in the process of switching medications. Between drugs, “I became a piece of furniture that he could step on or whatever; he totally ignored me,” she says. When his seizures were back under control, “he went back to his baseline.” She says epilepsy does not cause autism but can exacerbate it: “That’s why it’s so vitally important to treat epilepsy.”
For children such as Kevin, however, that is easier said than done. The procedure Ghatan performed is approved for treating adults with seizures under limited conditions, such as when the seizures arise from a known but inoperable region. But Kevin’s seizures seemed to start all over his brain, so Ghatan delivered a pulse to Kevin’s thalamus, which acts as a relay center in the brain, as part of a ‘palliative treatment.’ Ghatan got the idea from trials with deep brain stimulation, which some doctors use to treat Parkinson’s disease, obsessive-compulsive disorder and, in rare cases, autism. A clinical trial in 2010 showed that stimulating the thalamus decreases the frequency of seizures in adults who have not responded to other treatments.
The approach presents problems for someone Kevin’s age, however. It is not approved for children in part because their skulls are still growing. And any brain surgery always involves risks, such as infection, brain bleeds and permanent damage. Before the surgery, Ghatan’s team scanned Kevin’s brain to map out a path for the electrodes, which they inserted more than 6 inches into his brain, through regions responsible for thought, planning and memory, to the thalamus. The day of the surgery, they aligned this route with a new brain scan taken after they had immobilized Kevin’s head in a vise. A robot then lined the electrodes up to follow the route with exacting precision. But as the doctors cut into Kevin’s skull, any excess bleeding or loss of cerebral spinal fluid could have shifted the position of his brain — and the desired path for the electrodes — off course.
Still, Ghatan had seen promising results. One 14-year-old boy Ghatan treated had experienced as many as 30 seizures a day, even after surgeries in which portions of the boy’s brain had been sliced and removed. Detecting seizures and stimulating his brain with one electrode in the cortex and one in the thalamus brought his seizures down to an average of about one a day, Ghatan reported last year. Ghatan has also implanted the device in 10 autistic children, 4 of whom, like Kevin, have at least one electrode in their thalamus.
Seizures tend to originate in the cortex, but Kevin’s thalamus proved so active that Ghatan and his team decided to connect two thalamic electrodes instead. They packed two additional cortical wires, which they’d placed above an unusually dense tangle of blood vessels, into the thin gaps between the device and Kevin’s skull — in case they decided to use them later.

Risky business: Kevin’s surgery is not approved for children but may be his last chance to get his debilitating seizures under control.
Given the risks, experts caution that epilepsy surgery is intended to treat only seizures. Autistic individuals who have only occasional seizures are unlikely to benefit. “We treat epilepsy pharmacologically, surgically and then behaviorally — and we treat autism behaviorally, pharmacologically and never surgically,” says Roberto Tuchman, director of neurology at the Nicklaus Children’s Hospital in Weston, Florida.
Still, says Berg, for some autistic people, surgery may offer a last hope. “What scares me are centers that are just surgical centers, [where] it’s like, ‘I’ve got a hammer — come on, nails,’” she says. But “there are some patients for whom nothing seems to be working: You’ve gone through the drugs; you’ve gone through the diet; maybe you’ve tried cannabidiol, or the medicinal recreational version of marijuana; you’ve done prayer therapy; you’ve done everything.”
A
s the surgery concludes and the doctors peel away the sheets, Kevin emerges, looking thin and younger than his 12 years. Ghatan unfastens the vise and holds Kevin’s shaved head gently in the crook of his arm as he bandages it. An almost imperceptible bulge on the boy’s skull conceals the two handfuls of electronics and wires on which his parents and surgeons are pinning their hopes.Ghatan leaves the operating room and takes an elevator to meet Kevin’s parents and brother. “I still have a hundred years’ worth of anxieties,” he says. But when he greets the family, he gives them the good news that the surgery went well.
Lightner, too, tries to temper her expectations after Ghatan delivers his report. “We’ve looked forward to this day for so long, but it’s kind of anticlimactic because we have so much further to go,” she says. “It’s not like he’s going to wake up tomorrow and his seizures will be gone.”
That night, Kevin has so many seizures that his neurologist turns on the electrical pulses the following day. It usually takes weeks for the device to see enough seizures to begin to predict them. But almost immediately, Kevin starts having seizure-free days; he is released from the hospital two days after his procedure. Fields predicts that this is a post-surgery “honeymoon period,” and she proves to be right: Slowly, the nighttime seizures return. But they stop at between 3 and 20 a night — nowhere near the previous frequency of 50.
In the following months, Kevin comes to see Fields every four weeks. He seems more independent each time and ultimately stuns her by walking into her office unassisted in June. “Every time he comes to see me, it’s been like a new awakening,” she says.
Thanks to the implant, Fields is able to chart Kevin’s seizures and tweak the device’s settings and his medications accordingly. Lightner also tracks obvious seizures and can confirm an ongoing seizure by placing a magnet on Kevin’s head to flag it in the device’s recordings. This feedback helps Fields to check whether the device is detecting all of Kevin’s seizures. It seems to be working so far, although Kevin may be having seizures that are undetectable in the thalamus and that Lightner may not notice.

New start: Kevin’s parents and brother, Brian, hope the surgery will bring Kevin back to where he was before frequent seizures overwhelmed his brain.
More than four months after the surgery, on a sweltering July weekend, Lightner’s uncertainty about Kevin’s future shifts to hopeful excitement. The family takes refuge in an air-conditioned movie theater to watch a film about Apollo 11, the first moon landing. Kevin would typically have slept through the movie or been carried out to the car as he had a seizure, while his brother, Brian, continued to watch. Not this time.
At one point during the film, Kevin starts to applaud loudly. Lightner is initially uncomfortable, she says; she does not like to redirect Kevin’s outbursts and movements, but she also hates to disrupt others in the audience. To her surprise, however, the others start to clap as well: It turns out to be the moment when Neil Armstrong utters the famous words, “The Eagle has landed.” Kevin continues to clap at all the appropriate times, his mother says.
The following night, Lightner tells Kevin to “up, up, up, up,” as she always does, so she can help him get dressed for bed. “Up,” he repeats, uttering his first word in years, she says. “Up, up,” he says again. And then he stands.